An 80-year-old woman came to my office for a second opinion after being told four months earlier that she needed cataract surgery by another surgeon. She had already seen another ophthalmology practice and left the visit feeling uneasy. What bothered her most was not necessarily the recommendation for surgery itself, but the feeling that her prior history of LASIK had not been carefully considered during the discussion.
That feeling stayed with her.
To many people outside medicine, this may seem like a small detail. But for patients, confidence matters. They want to feel heard. They want to know their doctor sees the whole picture, not just the cataract.
So she decided to seek another opinion before moving forward.
During her examination, her corrected vision measured 20/20 in the right eye and 20/30 in the left. She did indeed have moderate cataracts in both eyes, and signs of prior LASIK surgery were clearly visible on corneal examination.
But something else immediately stood out.
Her optic nerves showed cupping with a cup-to-disc ratio of approximately 0.7 in both eyes. Her eye pressure was also elevated, measuring 30 in the right eye and 21 in the left.
At that point, the conversation shifted completely.
The cataracts were not the most urgent issue.
The larger concern was glaucoma.
The Silent Thief
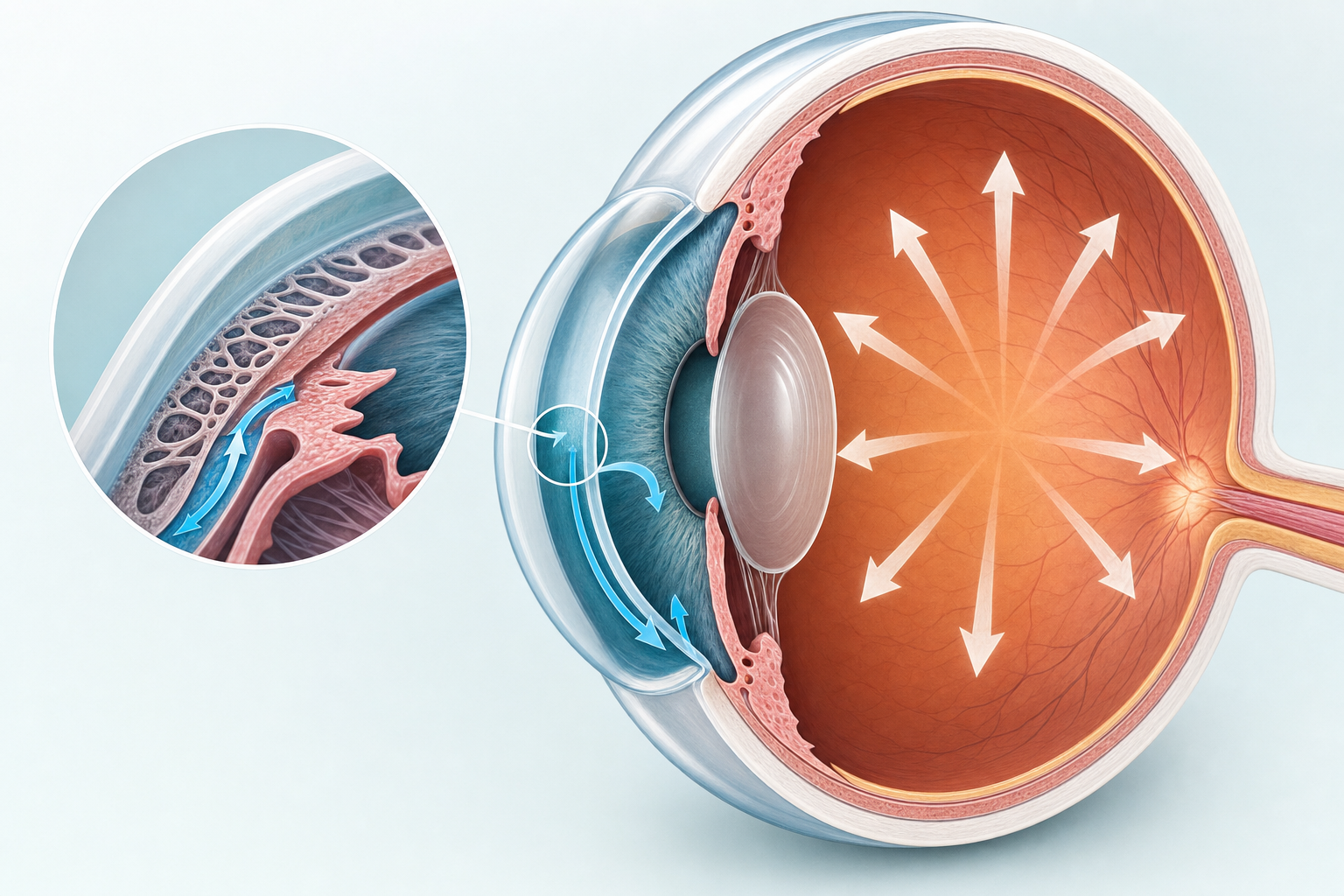
Glaucoma is often called the "silent thief of sight" because patients may lose peripheral vision slowly over time without noticing major symptoms early on. Unlike cataracts, which usually cause blurry or hazy vision that patients can see and describe, glaucoma can quietly damage the optic nerve before patients realize anything is wrong.
In her case, the combination of elevated eye pressure and advanced optic nerve cupping strongly suggested underlying glaucoma that had not yet been fully evaluated.
I explained to her that although cataract surgery may eventually become appropriate, it would be premature to focus on the cataracts without first understanding the health of the optic nerve and the severity of her glaucoma.
That distinction matters tremendously.
When Two Conditions Require Different Strategies
When patients have both cataracts and glaucoma, surgical planning often changes. Rather than performing cataract surgery alone, we frequently consider combining cataract surgery with minimally invasive glaucoma surgery, commonly called MIGS, to help lower eye pressure and reduce long-term glaucoma risk.

Equally important, her vision was still functioning quite well. At 20/20 and 20/30, she was not experiencing major daily limitations from the cataracts themselves. She was not struggling significantly with driving, reading, or routine activities. In medicine, the presence of a cataract alone does not automatically mean surgery is necessary. The decision should always connect back to how much the condition is truly affecting a patient's quality of life.
That became the focus of our discussion.
Instead of rushing toward surgery, we arranged for a full glaucoma evaluation including additional testing to better understand the extent of optic nerve damage and determine the safest long-term treatment plan.
The Value of Slowing Down
Cases like this highlight an important reality in ophthalmology: sometimes the most valuable decision a doctor can make is slowing down.
Modern medicine often moves quickly. Patients may feel pressure to "fix" anything visible on an exam, especially when surgery is involved. But good medical care is not about finding the fastest procedure. It is about identifying the true problem and treating the patient as a whole person.

Trusting Your Instincts
Psychologically, this patient's instincts were also important.
Patients sometimes worry they are being "difficult" if they question a recommendation or seek another opinion. In reality, uncertainty is part of being human. When a patient senses that something has not been fully addressed, that feeling deserves respect, not dismissal.
Interestingly, her decision to pause and seek another opinion may have protected her vision in the long run. Had the focus remained only on cataracts, the more dangerous issue, possible progressive glaucoma, could have continued silently in the background.
The Bigger Picture
There is also a philosophical lesson here about clarity.
People often think blurry vision comes only from cataracts because cataracts are visible and familiar. But not all vision loss comes from what clouds the eye. Sometimes the greater danger is damage occurring quietly behind the scenes.
Life works that way too.
The most obvious problem is not always the most important one. Sometimes we become fixated on what is easiest to see while missing the deeper issue quietly causing long-term harm.
In ophthalmology, that deeper issue can be glaucoma.
That is why careful examination matters. That is why listening matters. And that is why second opinions can be valuable, especially when something does not feel completely right.
For patients, the takeaway is simple: cataract surgery should never feel rushed simply because a cataract exists. Surgery decisions should be individualized, thoughtful, and connected to your symptoms, visual needs, and overall eye health. And sometimes, the best surgical decision is realizing surgery is not the first step at all.
Related Reading
- Do I Really Need Cataract Surgery?
- When the Surgeon Says Wait
- Second Opinion on Cataract Surgery: When and Why
- A Second Opinion That Changed the Conversation
- Glaucoma Care
- Glaucoma and Cataract: Combined Treatment
- How to Choose a Cataract Surgeon
- Cataract Surgery and Diabetes: What You Need to Know
- Complex Cataract Surgery: When Your Case Isn't Routine
- Macular Degeneration: Wet vs Dry
- Floaters, Flashes, and When to Worry