How Glaucoma Changes the Surgical Conversation
When a patient has only cataracts, the main decision is about the lens: which implant best matches their visual goals and lifestyle. When glaucoma is also present, the decision tree expands.
First, I think about lens selection differently. Multifocal lens implants, the ones that provide both distance and near vision, divide incoming light among multiple focal points. That division reduces contrast sensitivity slightly. For a patient with healthy optic nerves, this tradeoff is usually negligible. But for a patient who already has peripheral vision loss from glaucoma, even a small reduction in contrast can make a meaningful difference in how they see in low light, how well they perceive edges and depth, and how comfortable they feel driving at night.
This does not mean patients with glaucoma cannot have premium lenses. It means the decision requires more nuance. A patient with early, well-controlled glaucoma and minimal visual field loss may do perfectly well with a Vivity extended depth-of-focus lens. A patient with moderate field loss may be better served by a monofocal implant that preserves full contrast. The key is matching the lens to the whole eye, not just the cataract.
Glaucoma does not disqualify you from cataract surgery. But it does change which lens implant will give you the best functional result. The surgeon who manages both conditions is the one best positioned to make that recommendation.
Second, I think about the pupils. Many patients on long-term glaucoma drops, particularly certain classes of medications, develop pupils that do not dilate well. A small pupil makes cataract surgery more challenging because the surgeon needs to see and access the lens through the pupil. This is not a barrier to surgery, but it requires additional steps and experience. I may use devices to gently expand the pupil or adjust my surgical technique to work safely in a tighter space.
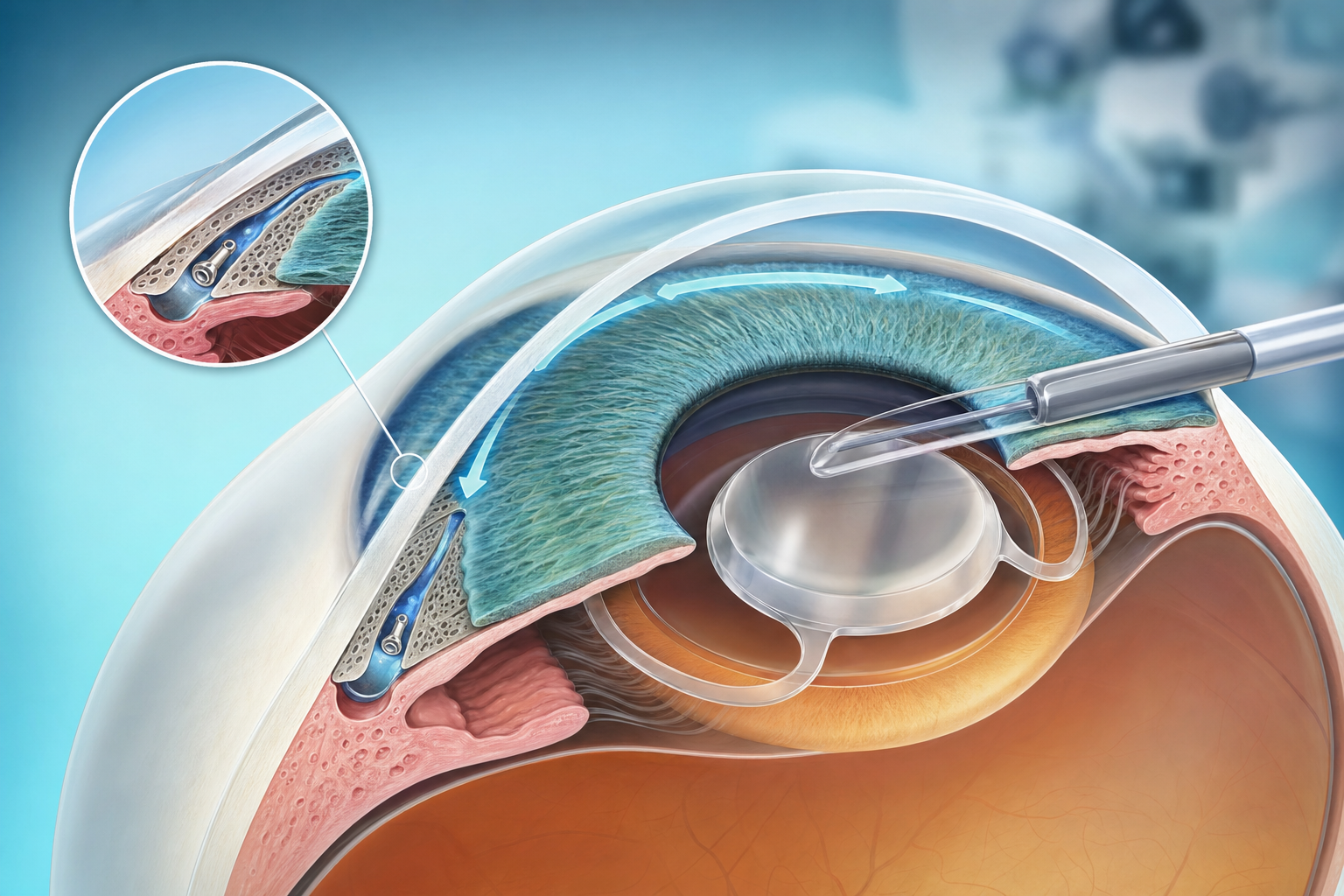
Third, I consider the opportunity for combined treatment. This is where the conversation gets most interesting for patients.