Wet Macular Degeneration: The Urgent One
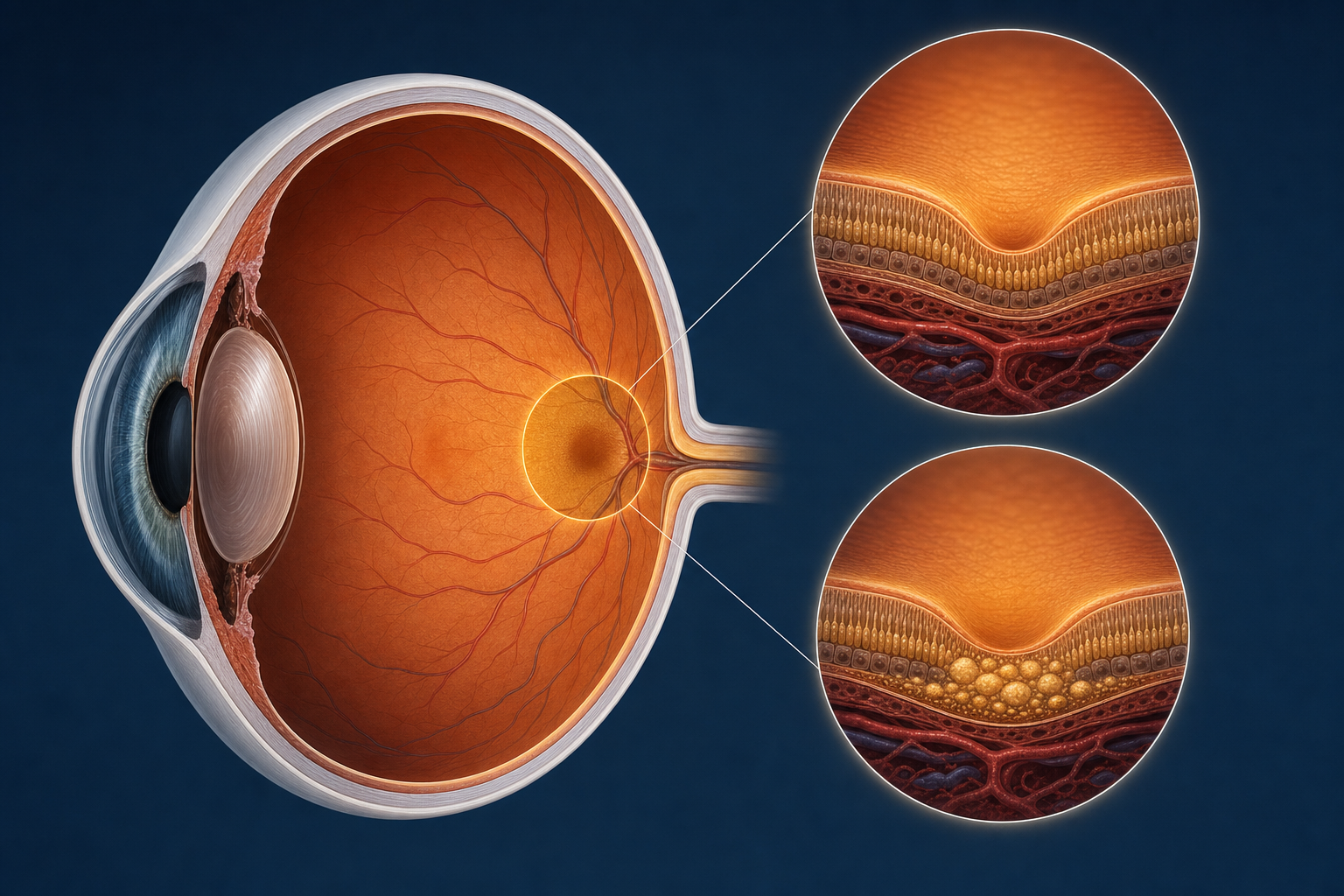
Wet AMD is different. It occurs when abnormal blood vessels grow beneath the retina in a process called choroidal neovascularization. These vessels are fragile. They leak fluid and blood into the retinal layers, causing rapid swelling and distortion of the macula.
The symptoms of wet AMD tend to appear suddenly. A patient may notice that straight lines look bent, that a dark spot has appeared in the center of their vision, or that their reading vision has deteriorated sharply over days or weeks. This is a fundamentally different timeline than dry AMD, which unfolds over years.

Central vision loss from macular degeneration often affects reading first. Patients describe the words becoming harder to track, letters blending together, or a dark smudge over the page.
Wet AMD accounts for only about 10 to 15 percent of macular degeneration cases, but it is responsible for the majority of severe vision loss associated with the disease. The good news is that it is treatable. Anti-VEGF injections, medications delivered directly into the eye, block the growth factor that drives the abnormal blood vessel formation. These injections can stop the leaking, reduce the swelling, and in many cases stabilize or even improve vision.
The most commonly used anti-VEGF medications include ranibizumab (Lucentis), aflibercept (Eylea), and faricimab (Vabysmo). Newer options like faricimab have the advantage of longer duration, meaning some patients can go two or three months between injections rather than receiving them monthly.
The key with wet AMD is speed. The sooner treatment begins after symptoms appear, the better the visual outcome. Waiting weeks or months allows the leaking blood vessels to cause more damage to the retinal tissue, and that damage may be permanent.
"He told me there was nothing they could do. But he never told me I had the kind that responds to treatment. I lost three months."