The Procedure Itself
The entire surgery takes about 8 to 15 minutes per eye. You are awake. You are comfortable. You are lying back with a light drape over your face, with an opening over the eye being treated. A small device holds your eyelids open gently so you do not have to worry about blinking.
What you see during surgery is not what people imagine. There are no instruments coming toward you. There is no blade visible. You see a bright light from the microscope above, sometimes with soft, shifting colors. Some patients describe a kaleidoscope. Others see a warm glow. Nobody watches the surgery happen from their perspective. The light above is bright enough to obscure everything else.
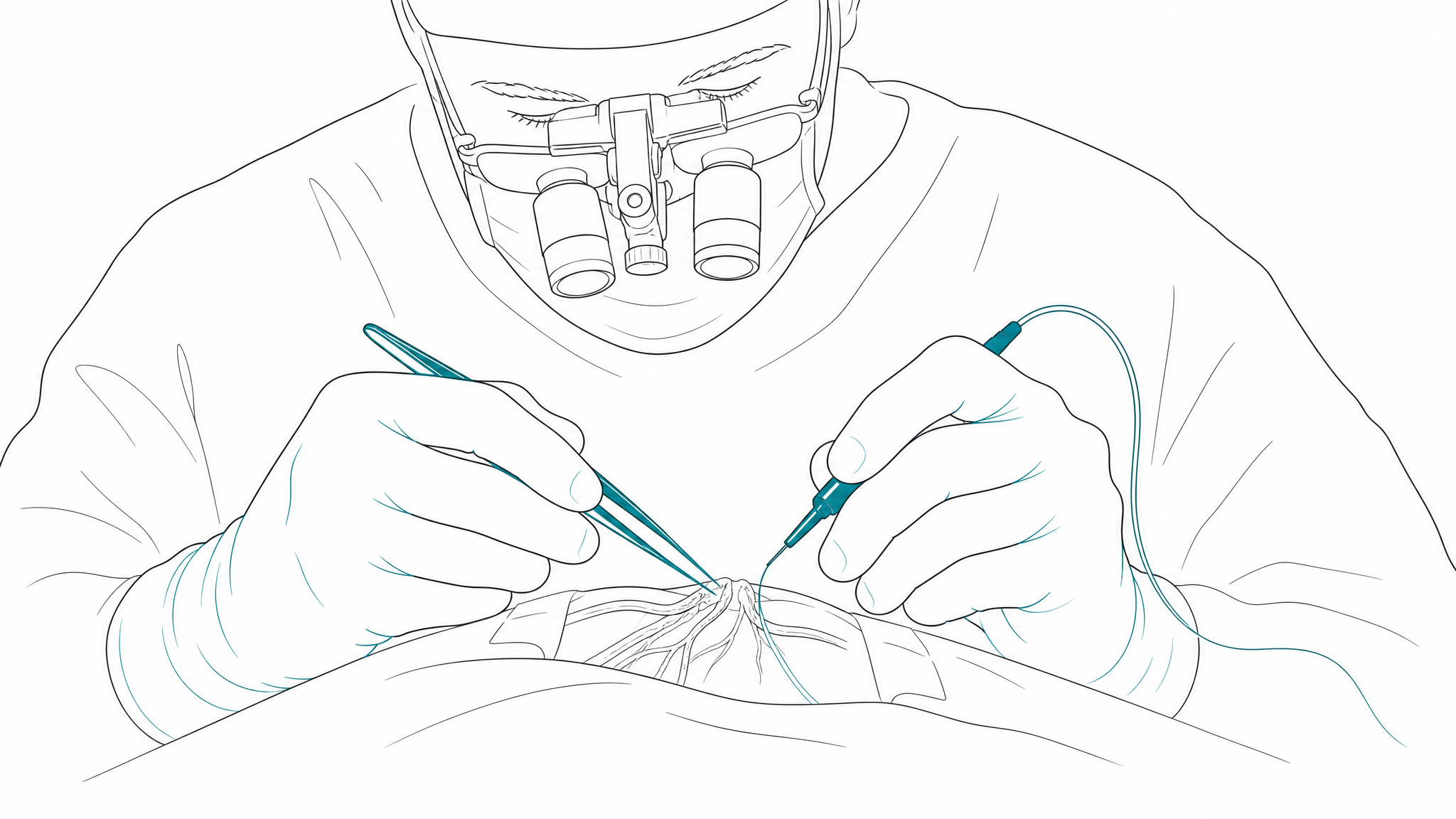
Here is what I am doing during those minutes. First, I create a tiny incision in the cornea, typically about 2.2 millimeters. This incision is self-sealing, which means no stitches in most cases. If we are using the femtosecond laser, this step and several others are performed by the laser with computer-guided precision before I begin the manual portion.
Next, I make a circular opening in the thin capsule that holds the cataract. Think of this capsule as a clear bag. The cataract, your clouded natural lens, sits inside it. I need to open the front of the bag to reach the cataract while leaving the back intact to support the new lens implant.
Then comes phacoemulsification. This is the technical name for what most people call "breaking up the cataract." An ultrasonic handpiece vibrates at an extremely high frequency, emulsifying the cloudy lens into tiny fragments that are simultaneously suctioned out through a small tip. The entire cataract is removed through that original 2.2-millimeter incision.
"The technology is remarkable, but it is not the technology that determines your outcome. It is the judgment behind it."
Once the cataract is removed, the capsular bag is clean and empty. This is where your new lens goes. The intraocular lens, or IOL, is folded and inserted through the same small incision. Once inside the eye, it unfolds and is positioned precisely in the capsular bag. This is the lens you will see through for the rest of your life.
The incision is checked for seal, and in most cases, no sutures are needed. A protective shield is placed over the eye, and you are done.