What the Exam Looks Like
When you come in for evaluation of new floaters or flashes, the most important part of the visit is a dilated eye exam. I place drops in your eyes to widen the pupils, which allows me to see the retina clearly from the center all the way to the far periphery where tears are most likely to occur.
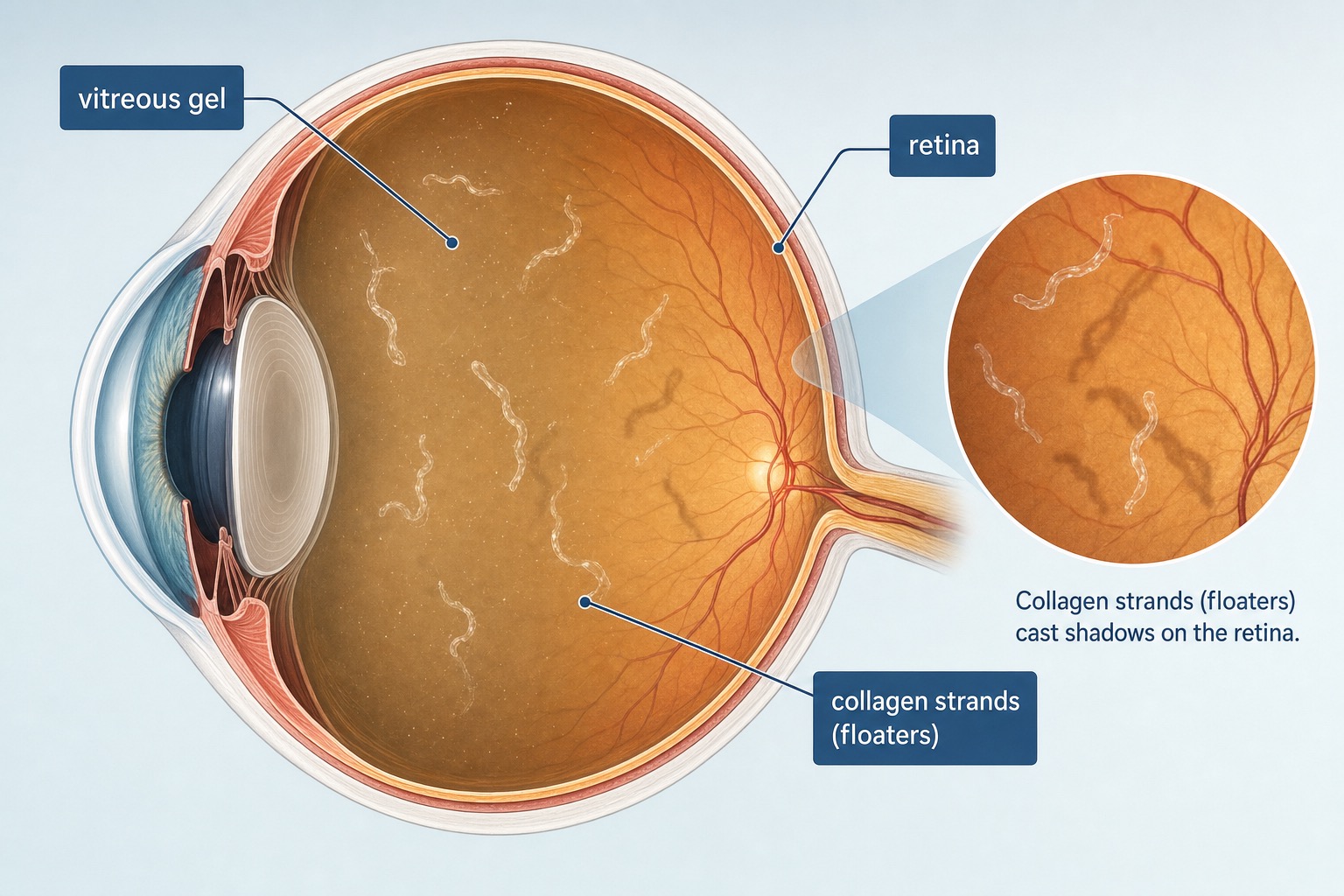
Using specialized lenses and a bright light, I examine the retinal surface in detail. I am looking for tears, thin spots, areas where the vitreous is still attached and pulling, and any signs that fluid has started to accumulate behind the retina.
The exam takes about 15 to 20 minutes once the eyes are dilated. It is painless, though the light is bright. Your vision will be blurry for several hours after dilation, so you will want to have someone available to drive you or plan to wait until the drops wear off.
If I find a retinal tear, I can often treat it the same day with laser. The laser creates a controlled area of adhesion around the tear, essentially welding the retina down and preventing fluid from getting underneath. The procedure takes a few minutes, is done in the office, and most patients feel only a mild sensation during treatment.
If the retina looks healthy and the vitreous is simply separating in the expected way, I send you home with reassurance and a clear set of instructions about what to watch for in the coming weeks. In some cases, I will ask you to return in four to six weeks for a follow-up exam, because a small percentage of retinal tears develop in the weeks after the initial vitreous separation, not during it.

A dilated exam is the single most important step when evaluating new floaters or flashes. It allows the surgeon to see the entire retina, including the far periphery where tears most commonly occur.