What Changes When You Wait
The most immediate consequence of waiting is the one patients already feel: declining vision. But the changes happening inside the eye matter just as much, because they affect the surgery itself.
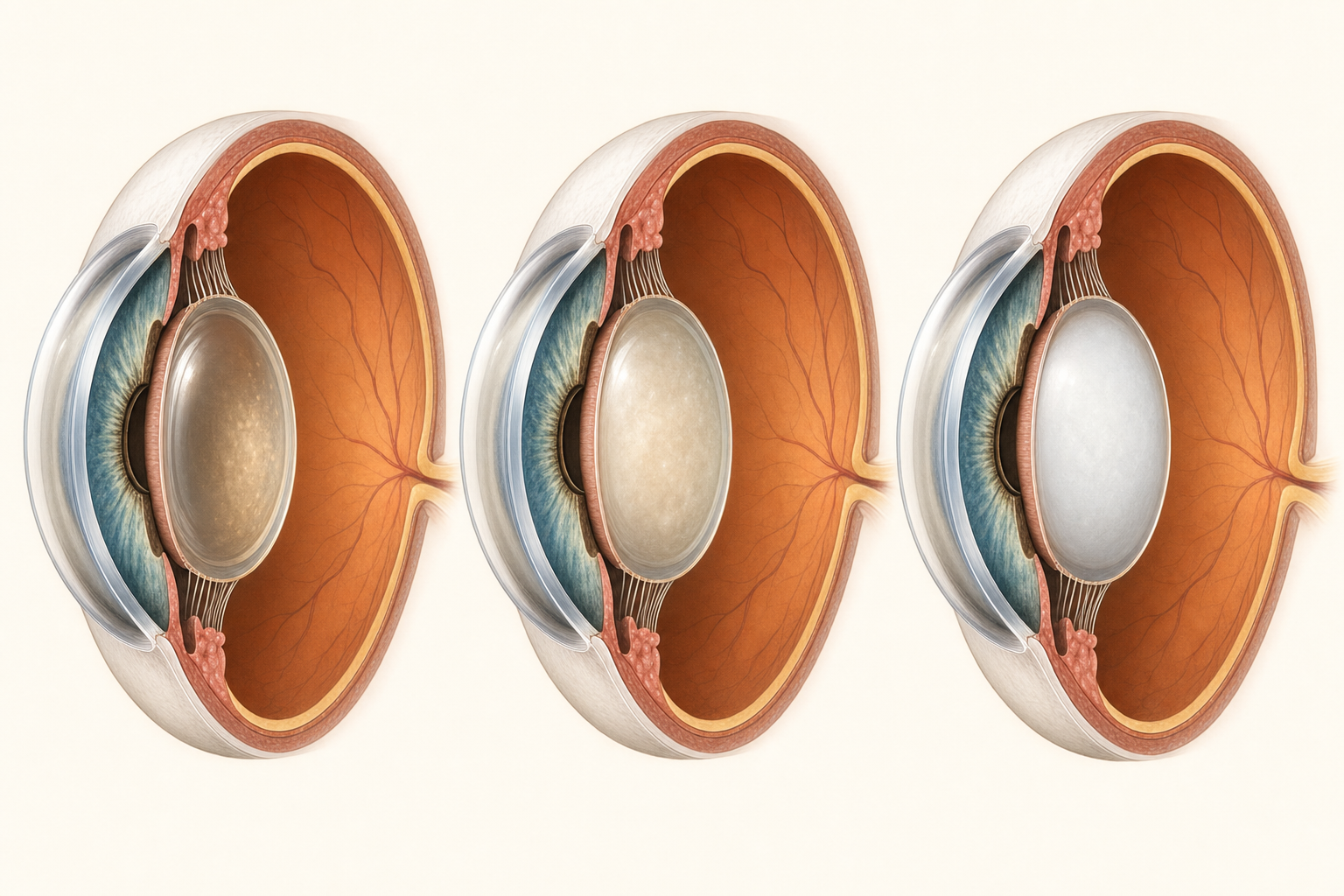
As a cataract progresses from early to dense, the lens becomes harder, more opaque, and significantly more challenging to remove safely.
The lens gets harder.
In early cataract surgery, the lens material is soft. It breaks apart easily with the ultrasonic energy we use during phacoemulsification. The surgery is smooth, controlled, and efficient. A dense cataract is a different procedure entirely. The lens is rock hard. It requires more energy, more time, and more manipulation inside the eye. Every additional minute of ultrasonic energy means more stress on the corneal endothelium, the delicate cell layer on the inside of the cornea that keeps your vision clear.
The capsule is at greater risk.
The lens sits inside a thin, transparent membrane called the capsular bag. During surgery, we carefully open the front of this capsule, remove the cataract through that opening, and then place the new artificial lens inside the intact bag. When the cataract is dense, the forces involved in breaking it apart put the capsule under significantly more stress. The risk of a posterior capsule rupture, the most common serious complication of cataract surgery, goes up. An experienced surgeon can manage this, but the margin for error is smaller.
Measurements become less accurate.
Before surgery, we perform detailed measurements of the eye to calculate the correct power of the artificial lens. These measurements rely on light passing through the natural lens. When the cataract is dense, less light gets through. The readings become less reliable. This can affect the precision of your lens power calculation, which means a greater chance of needing glasses after surgery or even an additional procedure to fine-tune the result.
Waiting does not make surgery impossible. It makes surgery harder. And the harder the surgery, the less predictable the outcome.

