One of the most important lessons I have learned in ophthalmology is that medicine is not always straightforward. Sometimes situations that initially appear disastrous evolve into something far more nuanced once the full clinical picture becomes clear.
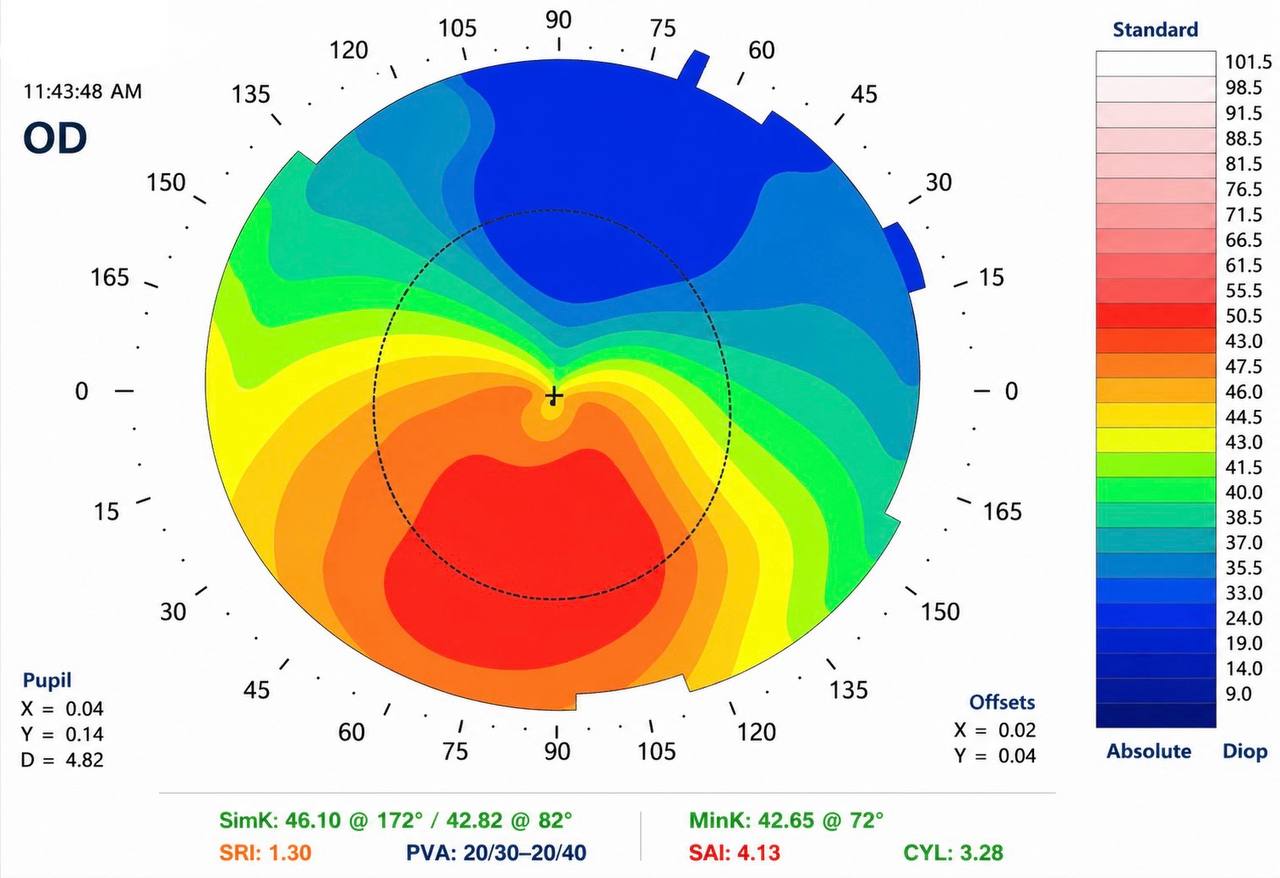
A 70-year-old patient recently came to my office for a second opinion after experiencing complications during cataract surgery performed elsewhere. Before his surgery, he had hoped to reduce his dependence on glasses. He specifically wanted a toric lens implant, a type of lens designed to correct astigmatism at the time of cataract removal.
During the original surgery, however, complications occurred. The posterior capsule, the delicate membrane that supports the lens implant inside the eye, ruptured. The toric lens could not be safely placed. A different lens was used instead. After surgery, his vision was dramatically worse, leaving him frightened, frustrated, and searching for answers.